
Chronic Pain
The Four Levels of Pain
Describes the four levels of pain and implications for chronic pain sufferers
Posted October 18, 2012
By definition, pain sucks. Along with death, failure and rejection, it is one of the things we humans fear the most. And many folks deal with it on a day-to-day basis, and the impact on their lives can be devastating. Pain is on my mind because I am finally wrapping up a three month bout with chronic pain (although in some lexicons, I had subacute pain--for definitions see here and here). Indeed, I have not blogged in that time because of the disruption to my life. In mid-July I started experiencing mild to moderate sciatic pain, which evolved by the end of the month into moderate to severe levels. The pain was some in my hip, but mostly down the side of my leg, from my knee to my ankle. I had trouble walking, lying down and sleeping, and it disrupted virtually every aspect of life. Ultimately, an MRI revealed a cyst that had formed off my L4-L5 disc, which was surgically removed in September (my surgeon thought, based on the MRI, it was a synovial cyst. It turned out not to be that, but some strange, unknown kind of cyst). I am happy to report that the situation has finally resolved itself, and I am now back to baseline.
Anyway, while I was managing this process, I found myself thinking a lot about pain, and observing the times in which I handled it reasonably well and other times that I handled it less well, and so I figured I would share my observations here. One thing that was helpful to me was to keep clear in my head the different levels of pain, which correspond to the four levels of mental architecture I depict here in this graphic and discuss here in this chapter, pages 71-80. The four levels are as follows: 1) sensory-motor; 2) affective; 3) imaginative; and 4) linguistic narrative.
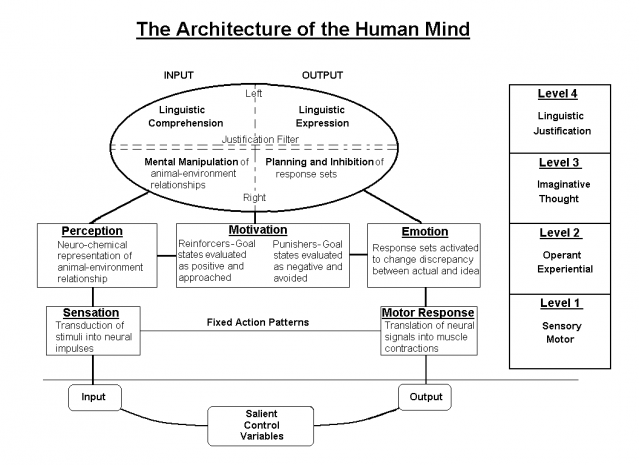
The sensory-motor level refers to the “raw feel” of the pain—in my case the raw experience of the throbbing in my hip or leg.
The affective level refers to my perceptual-emotional reaction to the pain. It was my perceived sense of what it was and my feelings about it. I disliked it and wanted to escape from it. As far as pain goes, the affective is closely tied to the sensory levels, but the two are actually separable. As the psychologist Nicholas Humphrey has documented in his writings, there are people who can have sensations of pain, but have no affective reaction to it. That is, they would feel something akin to the throbbing in my leg, but they would not have the intense emotional dislike of that feeling that I had.
The imaginative level refers to the images I had of what was causing the pain and imagined future sequence of interacting with the pain. As I experienced the pain, I had a picture in my head, first of something wrong with my hip and leg, and then as I learned more, I envisioned the cyst pushing against my nerves. I would also imagine myself in different places and at different times dealing with the pain. For example, some times during the day I would worry about how much it might hurt that night.
Finally, the linguistic narrative refers to my self-conscious talk about the pain, specifically my explicit theory of what is causing it, what it meant, and how it would unfold. I would go on line, read other people’s stories, and wonder what my ultimate storyline was going to be. Was my life changed forever? What if I never got better? Why do I think this happened? Is surgery a good thing? So on and so forth.
So what are the implications for chronic pain suffers? Well, the first thing is to realize that these levels are separate. One of the most notable elements of our conscious experience is that it seems to be a gestalt or a whole. Yet, it really is a tapestry of streams woven together. And these four elements, the raw sensation, the affective reaction, the imaginative thought patterns and linguistic narrative are elements that can be teased apart.
The second piece to keep in mind is that they interact and, very importantly, they feedback on one another. As sensory pain emerges, the affective reaction is of intense dislike and motivates the individual to escape. Images flood one’s consciousness and the narrator takes off, scripting what the experience means, and what it will mean in the future.
The third piece to keep in mind is that we humans have, potentially, much control over our mentation, especially our narrative, imaginative and affective processing. And this can make a huge difference in how the experience unfolds. Let’s start with a simple example. Like many children, when my daughter Sydney was younger she hated shots. While in the drs office one day when she was about five she heard needed a shot. As soon as she heard this, her whole face changed, she became affectively charged, and began crying and pleading with us that it not happen, that she did not want a shot. She suffered enormously—yet it was all at the level of affective, imaginative, and narrative thought. She did not experience the shot at the sensory motor level at all! Of course, as parents, we tried to calm her, change her narrative, distract her, motivate her, etc. Why? Because as every parent who has been there can see, the upper levels of thought play a huge role in how the experience unfolds.
And that brings me to my point about what I learned from my own experience, which supports what the research has found. There were times when my negative emotional reaction to the pain was high, when I imagined the damage the cyst was doing to my nerve, and when I thought about how unfair the situation was. These were the times when I suffered the most. In contrast, when I could muster the ego strength to lean into the sensory experience with acceptance, when I engaged in more pleasant centering imagery, and when I rescripted what the pain meant in my narrative, how I could (rather than could not) cope with it, and my hope for the future, my pain levels went way down.


As most clinicians now are aware, major advances have been made in helping people manage chronic pain via mindfulness training (for a well-known leader in this area, see here). These programs help individuals adopt a more accepting attitude about all aspects of their mentation, but especially creating a space for their sensory, affective and imaginative thought processes to play their course, but without judgment or reflective fear. In a related vein, other researchers have been looking at how to train folks to rescript the nature of their pain. A recent article by Phillips and Samson (2012) in Behavioral and Cognitive Therapy found that rescripting (which included both narrative and imaginative thought processes) initial images associated with their pain was very effective at reducing pain levels. The authors report, “The participants found it easy to rescript their distressing Index images. During rescripting, they reported dramatic reductions in emotion, negative appraisals, and pain. The clinically and statistically significant decrements in pain were found independent of reductions in emotion. The pain levels during rescripting were significantly below their basal levels, with 49% reporting no pain at all while viewing a rescripted image. These changes were not a function of image repetition”.
The bottom line is that pain sucks; however, as with so much in life, how one approaches it can make a huge difference in how the event unfolds. Learning acceptance and how to move one’s imagery and narrative toward adaptive places can be the difference between resilient adjustment and depressive despair. That said, I have a new found empathy and sympathy to all those who are suffering with pain on a daily basis and I wish them the very best in continuing to muster the courage to carry on in the most adaptive way possible.

