
Clinical/professional psychologists are engaged in a debate about what constitutes the best identity and training model for the field. Below re-post a blog I did on the APA Division 24 website for those PT readers interested in these issues.
In a recent blog on the APA Division 24 website, Dennis Wendt offers a thoughtful, clear, cautiously critical assessment of where the clinical scientist movement is and where it will be in 10 years. I share the concerns Dennis raises. In my view, he rightly predicts that “scientists and clinicians” will not become much closer via this model because they are rewarded by different mechanisms and often occupy different worlds. He also points to the complexities of practice as being fundamentally at odds with the needs of a researcher to design controlled studies. I also appreciated his suggestion that we need “a decade of clinical practice”.
Despite my agreements with many of his points, I do not think his analysis is fully successful because I don’t think it gets to the heart of the issue. Why? Because it frames the issues in more pragmatic terms, as opposed to the foundational identity issues; that is, I think deep confusions about what psychology is, what science is, and what psychological practice is (or should be) exist at the heart of the difficulties for the clinical scientist model. It is because of these reasons, which I elaborate more here on my Psychology Today blog, that I believe the clinical scientist model does not represent a viable model for the field.
To understand why, let’s start by being clear about what the clinical scientist model is. To do so, let’s take a brief detour and remind ourselves of our history, because issues of identity always relate to issues of history. First, let’s recall the birth of “psychology”. What defined it? In many ways, psychology’s identity and separation from philosophy was the application of the methods of science to empirically answer questions that were previously addressed solely via rational argument. So, as I note in Henriques (2013), much of psychology’s identity has been intertwined with the application of the scientific method. Now, fast forward a couple of decades and move to America, where, in the 1910s, 20s, and 30s, clinical psychology was born and psychologists began to enter into realms of application. What was our defining feature initially? We brought the methods of behavioral science to bear on questions of assessment and intervention. This largely translated into our role as emphasizing things like assessment and measurement (e.g., intelligence and aptitude testing) and playing a supporting role for institutions like the army and to health professionals like psychiatrists via analyzing questions using what might be called empirical behavioral science methodology. I raise this point because this represents the foundational identity for the current clinical scientist movement. This is clear when we contrast it to the other training models in clinical and professional psychology.
On the heels of WWII in the late 1940s there was a huge push for the services of more and more mental health professionals, and ultimately it was recognized that a new identity was needed for clinical psychologists. As such, applied psychologists convened at the Boulder Conference, which gave rise to the scientist-practitioner model in clinical psychology. The societal push for psychologically informed mental health professionals continued and the practitioner side of the field continued to develop along with it. Three decades after Boulder, a group of applied psychologists argued that what was needed was a practitioner-first identity for the field. This was articulated at the Vail Conference through the full professional (practitioner-scholar) model. The Vail model was followed by the institution of professional schools, which, at best, had mixed consequences for the field. Nevertheless, what Vail definitely did do was legitimize the practitioner and related competencies as a viable identity for professional psychology.
The clinical scientist model of training can only be understood via this history. It exists as being explicitly defined against both the Scientist-Practitioner and Practitioner-Scholar models of training clinical psychologists. Historically, the kind of training the current clinical scientist model programs offer would simply have been on the science-side of the science-practice continuum. But that is not the kind of identity that current clinical scientists have of the field. Why? Because for them, clinical psychology means commitment only to empirical behavioral science methodology. It the historical positioning that allows us to see most clearly why the clinical scientist model that rejects the identity of a psychological practitioner that is distinct from the science. Keeping this history in mind, we can go to the current articulation of the clinical scientist model as specified by the Psychological Clinical Science Accreditation System to see this clearly. As stated on that website, the clinical scientist model and the PCSA System were created “to promote superior science-centered education”, ostensibly in contrast to the existing state of affairs. The system was “predicated on the assumption that public health will be served best by training clinical psychologists as scientists who will use their knowledge and skills to advance basic knowledge as well as to develop and evaluate more cost-effective interventions, assessments, and prevention strategies”. To be eligible for PCSA accreditation, programs must be PhD programs at “research-intensive universities” that “subscribe to an empirical epistemology”. The program must “provide the skills required for successful careers as research scientists in clinical psychology”. Indeed, the biggest determinant of evidence that a program is worthy of accreditation is that the program has “a consistent record of graduating clinical scientists”. Of particular note, they state “whereas some graduates of clinical science programs may pursue careers devoted primarily to practice, the programs judged to be of highest quality will be those that demonstrate convincingly that the majority of their students contribute significantly to advancing scientific knowledge” [italics added].
Anyone familiar with academic life at an R-1 university can see clearly the type of individual these programs are aspiring to produce: researchers who analyze data, publish articles, and get grants. Secondarily, they (begrudgingly) turn out clinical scientist technicians who apply empirical manuals to effect change. As far as I can determine, the word “practitioner” does not appear as part of the lexicon in the clinical scientist model.
With this review of the clinical scientist model, let us return now to Dennis’ concerns and reflect on whether one should be optimistic as to whether or not the clinical science movement will be the key to the effective resolution to the science-practice divide. In doing so, let’s begin with a question: “If a loved one of yours was having some serious psychological difficulties, say dealing with bulimia and depression, and I ask you, what are the competencies you hope that their health care professional would have, would you be more inclined to refer them to a practitioner whose primary identity is forming effective therapeutic alliances that foster understanding and adaptive change, or would you want to send your loved one to a researcher on eating disorders who was good at getting grants, and writing peer-reviewed papers?”
This question is the straightforward way of addressing the central question of this blog, which is: What is the proper foundational identity for clinical psychology? The PCSA position is that practice can be reduced to the methods of science. By their own description, clinical psychology is a science, seemingly just like social, developmental or personality psychology. Completely lacking from this perspective is the recognition of a systematic distinction between the science of psychology and the profession (Henriques, 2011).
My position, as a deep, lifelong student of psychology (trained in the Boulder Model and Director of a quasi-Vail model program), as a prior director of a randomized controlled clinical trial, as one who loves the science of psychology, and who has functioned as a basic psychological researcher, theorist, educator, and general practitioner, is that the PCSA offers a deeply misguided view of the field. My view is that the science of human psychology has a fundamentally different identity, role, and mission in society than that of the profession. The parallel is akin to the distinction between biology and medicine, as well as physics and engineering, and sociology and social work. Human psychology consists of disciplines like developmental, social, cultural, personality and cognitive specialties, among others. Human psychology is a scientific enterprise and fits within the pantheon of sciences, existing “above” biology and neuroscience, and “below” sociology. Human psychologists appropriately have identities as research scientists, scholars, and educators and their competencies are in getting grants, writing technical papers, and educating the public on a scientific understanding of the human condition.


In contrast, clinical, counseling and school psychology (i.e., licensed professional psychologists) operate in society in a fundamentally different way. The role of licensed psychologists is not simply in the scientific description and explanations of human behavior. Instead, their role is explicitly prescriptive. Professional psychology, of course, does require a scientific knowledge base from which to operate, and we certainly need research into psychopathology, psychological assessment and psychotherapy, among other domains. But the identity of professional psychology is neither primarily of science (i.e., a specialist in empirical behavioral research methodology) nor is it reducible to such methodology. Professional psychologists function as health service professionals and are given applied charges to improve the well-being of their patients/clients. Although it complements and informs human psychology, it is a radically different identity than that of human psychology. And we must understand it is a difference and identity that the clinical scientist model explicitly is defined against. The PCSA model collapses the two identities into one, folding them both into the “science” and claims we can reduce the practice professional dimension to the application of scientific methodology.
It is useful to note that there are remnants of the science-practice distinction, and it is a hierarchical one, with the division existing between knowledge generation via scientific methodology and the application of such knowledge. As stated on the PCSA website, the greater position is the generator of science. This is the academic who cuts through complexity and identifies the key variables and processes to effect change. The lesser position is the clinical science technician, who mechanically applies the insights to empirically determined situations. To clinical scientist folks, both positions are scientists, which is why the PCSA system doesn’t use the term “practitioner”.
My scholarly position is that all of this ultimately stems from psychology’s crisis of identity and its failure to effectively define its subject matter (Henriques, 2004). Because psychology has struggled so much with its identity, in many quarters it retreated to its methods, such that now the field is largely defined by its reliance on the scientific method (Henriques, 2013). This, however, is a weak intellectual position. Consider, for starters, that there are many disciplines (economics, anthropology, sociology, medicine) that rely on scientific methods, so this is hardly distinctive. In addition, the results of any method-based study yield data and information, which, alone, this is essentially meaningless. It is only when these data are connected to a network of theoretical and conceptual understanding that the data and information produced via the method gives us its value. In other words, it is not the method per se that is valuable, but how the results from the method mesh with our existing conceptual understanding.
The limitations associated with relying solely on data derived from the scientific method as a primary identity become even more complicated when we think of the prescriptive, value-based role of the professional psychologist. Consider the following questions: Is it helpful and appropriate to think of depressive conditions as diseases? Or should we view them as maladaptive learning patterns? Or perhaps as necessary aspects of being human? Should we, as practitioners, emphasize accurate self-knowledge and awareness or should we focus on feeling good, even if based on biases and illusions? Should we work to promote fully equal rights for transgendered individuals and strive to remove gender biasing language from our discourse? Is the professional psychologist model I advocate for here better than the clinical scientist model of the PCSA? There are endless examples of such questions.
Science and the scientific method per se are only peripherally related to such questions because they involve values, worldviews, and visions for the future. Yet, the questions and their answers relate centrally to mental health and our society’s understanding of the human condition. The point here is that with some reflection, it becomes apparent that our identity and the knowledge systems that we as clinical/professional psychologists need to be operating from cannot be fully reduced to empirical research methodology. The methods of science are wonderful tools and are essential for improving our knowledge systems, revealing new insights and reducing error. But scientific methodology is not the be all and end all of what it means to be a professional psychologist.
As I have been writing on for the last decade, we need to have a different view of science, one that emphasizes concepts and appropriately views methods as tools by which we build scientific concepts (Henriques, 2011; 2013). At an even broader level, we need to build a credible conceptual map of the discipline, one that clearly defines, first and foremost, the subject matter of the science of psychology and offers an integrative meta-theoretical framework for transforming the current pre-paradigmatic chaos into a comprehensible vision of animal behavior and the human mind (Henriques, 2003). The map of psychology I offer emphasizes two fundamental distinctions with in the field. The first fundamental distinction is between the basic science of psychology and human psychology. The former, with its focus on brain, mind, and behavior in general is natural science discipline that corresponds to the behaviors of animals. The latter is a social science discipline, and requires a fundamentally different epistemology (Henriques, 2004). The second key distinction is between the science of human psychology and the profession. This is what the map of psychology looks like from this view.
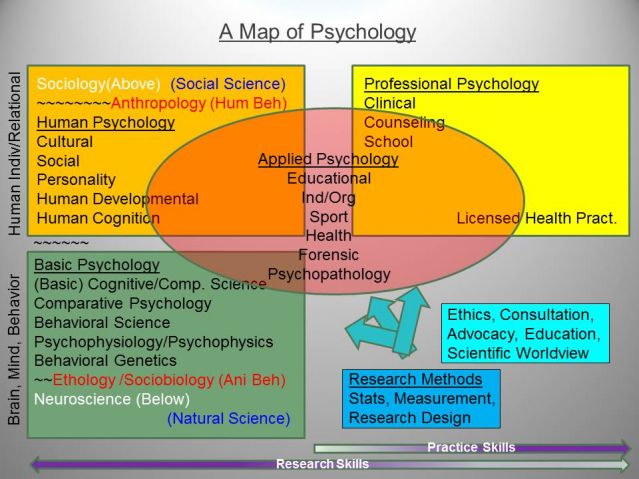
It is from the applied base of the science of human psychology that the identity of the professional psychologist emerges (Henriques and Sternberg, 2004). In this view, the professional psychologist is a category that does not just include “clinical”, but transcends the distinctions between clinical and counseling and child-clinical/school into a holistic view of a mental health profession. The identity of the integrated professional psychologist is one of a healer and promoter of human well-being, anchored to knowledge of human psychology, effective assessments and interventions justified by sound methodology, and a developed expertise that skillfully applies such knowledge to the uniquely idiosyncratic features that is a reality of every clinical situation.
This is the identity we promote at the program I direct (the James Madison University APA-Accredited Clinical-School Program). We call it a “Practitioner-Scientist” Model, whereby the emphasis is placed first and foremost on our identities as health service providers, and secondarily on psychological science. Moreover, rather than a scientifically reductive methodological fundamentalism, we teach a scientific humanistic philosophy, one that deeply emphasizes the need for a scientific approach, but also deeply recognizes the roles of values, subjectivity, and socially constructed meaning, both in terms of the work we do at the individual level and the larger global context in which the ideas we offer reside and have influence. It is this perspective, values, and skill set—which are prioritized over the competencies of analyzing large data sets via meta-analyses and structural equation modeling—that we believe are required of professional psychologists as health service providers. And, we believe, core faculty of training programs in professional psychology should model these competencies.
In the end, a solution that reduces practice to science is no solution at all. Moreover, to the extent clinical science programs openly and explicitly value researchers over practitioners (and, even worse, reduce professional practice to the mechanical-technical application of empirical research methodology), great damage is done the field of professional psychology. A solution to the infamous science-practice divide can only come if the professional practitioner has an identity as a psychological healer who is grounded in the science but is not synonymous with it. And to accomplish this, we need have trainers at the highest levels of the academy that embrace, exemplify and educate the next generation of professional psychologists in how to live it to its fullest potential.
References
Henriques, G. (2013). Evolving from methodological to conceptual unification. Review of General Psychology, 17, 168-173. DOI: 10.1037/a0032929
Henriques, G. R. (2011). A new unified theory of psychology. New York: Springer.
Henriques, G. R. (2004). Psychology defined. Journal of Clinical Psychology, 60, 1207-1221.
Henriques, G. R., & Sternberg, R. J. (2004). Unified professional psychology: Implications for combined-integrated doctoral training programs. Journal of Clinical Psychology, 60, 1051-1063.
Henriques, G. R. (2003). The tree of knowledge system and the theoretical unification of psychology. Review of General Psychology, 7, 150-182.

